Background: Fetal growth restriction (FGR) is the leading cause of fetal and neonatal mortality for Black women and a principal driver of racial disparities in fetal growth and birthweight outcomes. Yet, the high rates of FGR among Black women is not explained by FGR’s known antecedents (i.e., placental insufficiency, malnutrition) or risk factors. Moreover, interventions targeting such factors have been ineffective.
Central Question: Why do Black women have a disparate rate of fetal growth restriction & small babies?
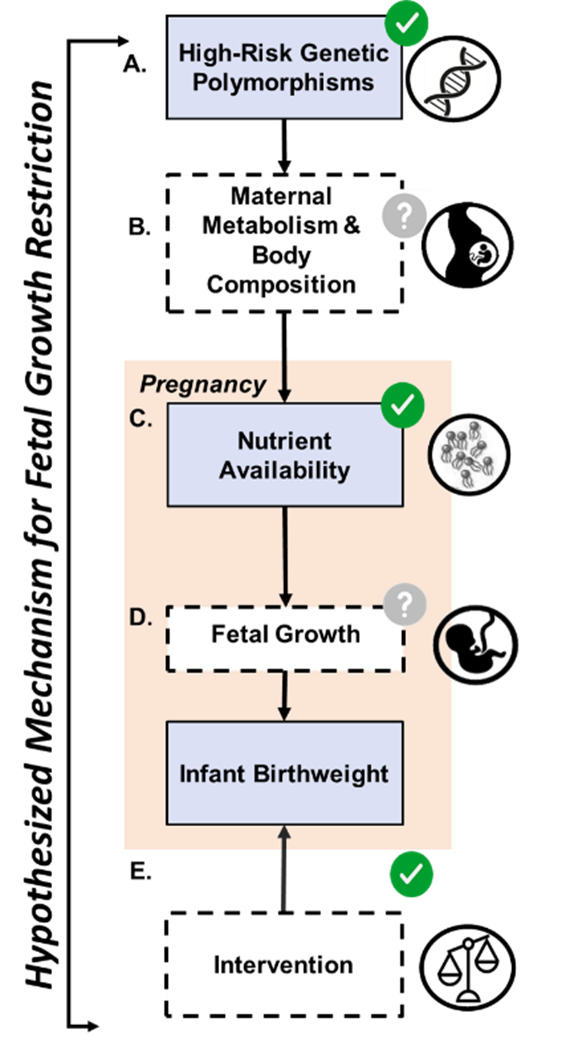
Scientific Premise: There is strong evidence that 1) FGR is a state of fetal nutrient deprivation, 2) high maternal lipid levels are required for fetal growth, and 3) on average, Black women have lower lipid levels during pregnancy, possibly due to genetic variations that are common among African ancestry and rare for other ancestries. Genetic variation may lead to higher lipid uptake in maternal tissues, fewer lipids for fetal growth, and ultimately to FGR.
Central Hypothesis: High risk genetic polymorphisms confer a particular maternal metabolic phenotype to some Black women, which interacts with maternal nutrient availability in late pregnancy to deprive a fetus of reaching its growth potential and development.
Scientific Approach: Uses applied genomics and metabolic phenotyping to define the role of genetics, maternal and placental lipids, and extrinsic exposures in FGR among Black women.
Project Innovation: This study investigates a modifiable, nutrition-based target to reduce FGR risk, paving the way for precision interventions.
Background: Chronic hypertension (cHTN) significantly increases the risk of preeclampsia (PreE), yet detection of PreE is often delayed, leading to severe outcomes. The diagnostic conundrum for patients who enter pregnancy with CHTN is, “Are increases in blood pressure and urine protein in patients with cHTN reflective of the normal physiology of pregnancy, or do the increases signal the development of PreE superimposed onto cHTN?”. As a result, evolving PreE in patients with CHTN is typically undiagnosed and unmanaged until more severe symptoms present, which is dangerous because PreE can rapidly evolve and lead to severe hypertension (BP ≥ 160/100 mmHg) or eclampsia.
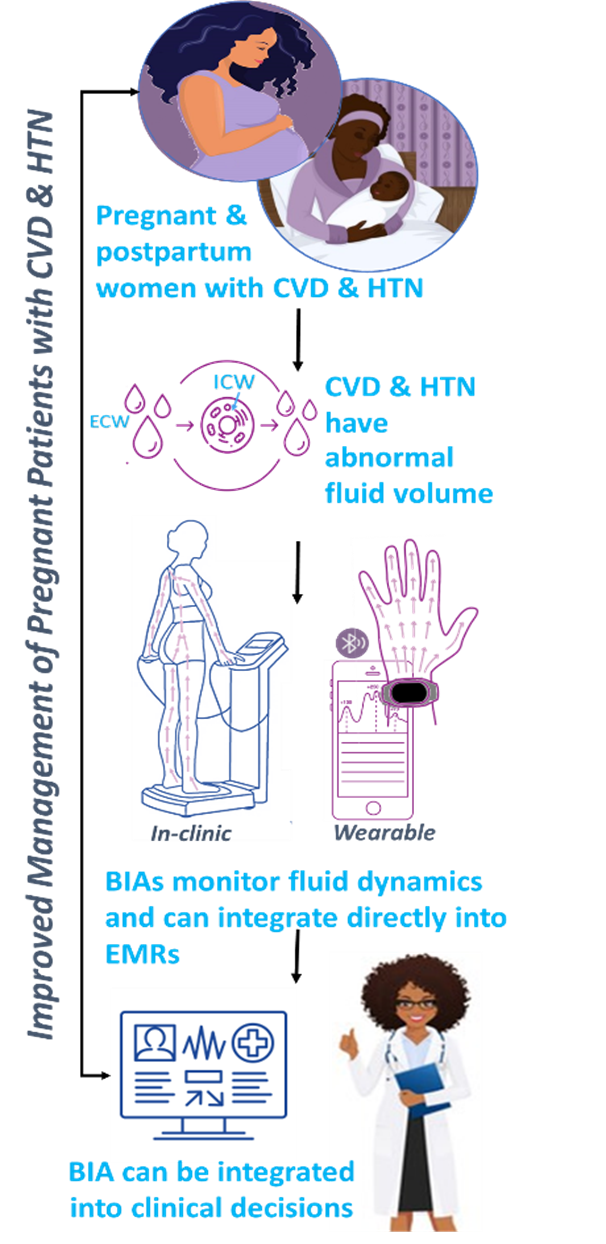
Central Question: Is fluid volume monitoring with a wearable device feasible and effective for detecting preeclampsia onset in pregnant and postpartum patients with CHTN.
Scientific Premise: In preeclampsia, fluid and electrolytes shift from the intracellular fluid (ICF) to the extracellular fluid (ECF) space, resulting in volume overload, which increases cardiac output and results in elevated blood pressure. ECF increases by up to 25% at PreE onset, whereas ECF remains constant in those with cHTN alone. This phenomenon has been measured using in-clinic bioimpedance techniques in normotensive pregnant patients who develop preeclampsia but has not been explored in those with cHTN.
Central Hypothesis: ECF volume will rise significantly in patients with cHTN who develop PreE and that both in-clinic and wearable bioimpedance devices can detect the relative change in ECF sufficiently enough to be used as a diagnostic indicator of PreE.
Scientific Approach: Using smartwatch-based wearable technology, we continuously monitor nighttime fluid dynamics during pregnancy to detect early signs of PreE before standard diagnosis. We also investigate the efficacy and feasibility of third-trimester ECF volume surveillance using a commercially available, wrist-worn, smartphone-based wearable device with a bioimpedance sensor.
Ongoing Projects:
- Evaluation of differences in fluid volume between those who develop PreE and those who maintain CHTN only.
- Characterizing the precision, stability, and reliability of wearable bioimpedance devices in pregnant and postpartum patients.
- Developing implementation strategies for integrating fluid volume measurements into clinical care for women with high risk for or diagnosis of hypertensive disorders of pregnancy.